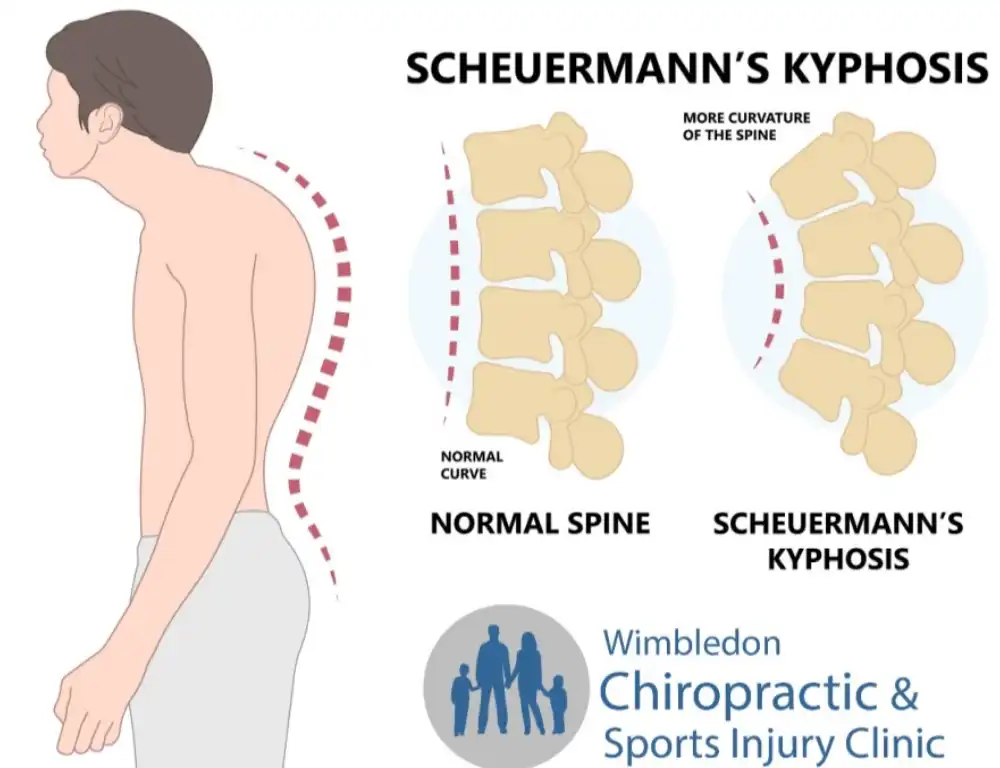
Scheuermann kyphosis, also known as Scheuermann disease, is characterised by structural deformity in the spine, particularly in the thoracic region.
Scheuermann manifests through a radiographic feature of nuclear end plate impressions. This is where the spinal discs' watery component intrudes into the bony vertebral bodies. Please think of this like the motor between two bricks breaking through the brick and cracking it. This causes the spinal vertebra structure (the 'brick') to become unstable and early disc degeneration (the morter).
This article delves into the specifics of the vertebra bone's shape after being damaged by the father of the disc, vertebral wedging, its radiological, x-ray, classification, and the implications for diagnosis and treatment.
Additionally, it explores recent findings on vitamin D deficiency in patients with Scheuermann disease, its association with adverse outcomes, and movement factors contributing to the condition.
Pathophysiology of Scheuermann Kyphosis
Scheuermann kyphosis primarily affects the thoracic spine, leading to a kyphotic curvature more significant than the normal range. The condition is believed to arise during adolescence, with genetic and biomechanical factors contributing to its development. The hallmark of Scheuermann disease is the wedging of at least three adjacent vertebrae by 5 degrees or more, leading to a pronounced kyphotic deformity.
Nuclear End Plate Impressions
Nuclear end plate impressions refer to the phenomenon where the nucleus pulposus, the inner core of the intervertebral disc, herniates into the end plates of the vertebrae. This intrusion weakens the structural integrity of the vertebral bodies, facilitating the characteristic wedging seen in Scheuermann kyphosis. This early disc degeneration often results in chronic pain and stiffness in the affected region.
Vertebral Wedging: Radiological Classification
The diagnosis and assessment of Scheuermann kyphosis heavily rely on radiological evaluation. Vertebral wedging is a critical feature that aids in diagnosing the severity and progression of the condition. The classification of vertebral wedging is based on the degree and type of wedging observed.

Degrees of Wedging
- Grade I: Mild wedging with less than 5 degrees of anterior wedging per vertebra.
- Grade II: Moderate wedging with 5 to 10 degrees of anterior wedging per vertebra.
- Grade III: Severe wedging with more than 10 degrees of anterior wedging per vertebra.
Types of Wedging
- Type I: Uniform wedging across the affected vertebrae, typically seen in earlier stages of the disease.
- Type II: Asymmetrical wedging where the degree of wedging varies between adjacent vertebrae.
- Type III: Mixed pattern with uniform and asymmetrical wedging areas, often indicating advanced disease with significant structural compromise.
Key Findings from the Study
The study reviewed the medical records of 11,277 patients with Scheuermann's disease. Of these, 1,024 patients (9.08%) were identified as deficient in vitamin D. However, only 1,421 patients (12.6%) had their vitamin D levels tested. Among those tested, a significant 72% were found to be deficient in vitamin D.
This highlights a potential oversight in managing Scheuermann's disease, where vitamin D levels are not routinely monitored.
Implications of Vitamin D Deficiency
Vitamin D plays a crucial role in bone health and metabolism. Deficiency in vitamin D can exacerbate the structural weaknesses in the spine caused by Scheuermann's disease, potentially leading to increased pain, deformity, and a higher likelihood of requiring surgical intervention. The study's findings suggest that routine screening for vitamin D levels should be considered in the management plan for patients with Scheuermann's disease to identify and address deficiencies early. This is more important in climates and multicultural areas like the United Kingdom or London, where we are based, as the statistics say that 1 in 4 people in the UK are likely to be low on vitamin D at any time.
Recommendations for Clinical Practice
- Routine Screening: Regular vitamin D level assessments in patients diagnosed with Scheuermann's disease can help identify deficiencies that may contribute to worsening symptoms and adverse outcomes.
- Supplementation: For patients who are deficient, vitamin D supplementation should be considered as part of the comprehensive treatment strategy to support bone health and potentially mitigate disease progression.
- Further Research: Continued research into the relationship between vitamin D levels and Scheuermann's disease outcomes is needed to establish definitive clinical guidelines and improve patient care.


Biomechanical Factors in Scheuermann Kyphosis
A review titled "Current Concepts on Scheuermann Kyphosis: Clinical Presentation, Diagnosis, and Controversies Around Treatment" (2012) highlighted several biomechanical factors that could contribute to the aetiology of Scheuermann's disease. One significant biomechanical factor is hamstring contracture, commonly observed in patients with Scheuermann's kyphosis.
Impact of Hamstring Contracture
Hamstring contracture impedes normal pelvic inclination during trunk flexion. This condition causes repeated flexion forces to concentrate through the thoracic spine, leading to progressive anterior wedging of the thoracic vertebrae. According to research by Ogden et al., asymmetric biomechanical stress on the vertebral bodies alters the remodelling response, contributing to the development of kyphosis.
Biomechanical Theory of Kyphosis
Kyphosis (upper back hump) results from an imbalance of the load supported between the front and back elements of the spine. It has been proposed that treatment with bracing in patients with thoracic hyperkyphosis could produce a posterior displacement of the centre of gravity and load axis, leading to the disappearance of anterior vertebral wedging. This supports the biomechanical theory of the origin of Scheuermann's disease. It stands that if picked up early enough, the humping deformity may be cancelled out in some shuermanns cases. But radiographic analysis should be sorted to confirm boney changes to indicate whether both treatment and bracing maintenance may be required over just regular self-lead physical Therapy.
Integrating Biomechanical and Nutritional Treatment Approaches
Considering Scheuermann's disease's biomechanical and nutritional aspects, a combined treatment approach may offer the best outcomes for patients.
Mechanical or Manual Treatment
- Physical Therapy: Targeted exercises to address hamstring contracture and strengthen the spinal musculature.
- Bracing: Use of thoracolumbar orthosis to correct spinal alignment and reduce anterior vertebral wedging.
- Manual Therapy: Techniques such as spinal manipulation and mobilisation to improve spinal mechanics and alleviate pain.